Why Getting Dental Care in New Jersey Is So Hard
It is not one problem. It is two systems failing at the same time.
When both systems break down at the same time, the people who need care most are the ones who fall through first. And a safety net that was built for occasional gaps is now absorbing the weight of two structural failures at once.
Below, you will find the full picture of each system, the data behind it, and a growing collection of stories, myths, and answers from real life in New Jersey.
What The Numbers Show
Here is what dental access actually looks like in New Jersey right now.

You Probably Think This Does Not Apply to You. Read This Anyway.
Here are four people in New Jersey. All of them [...]
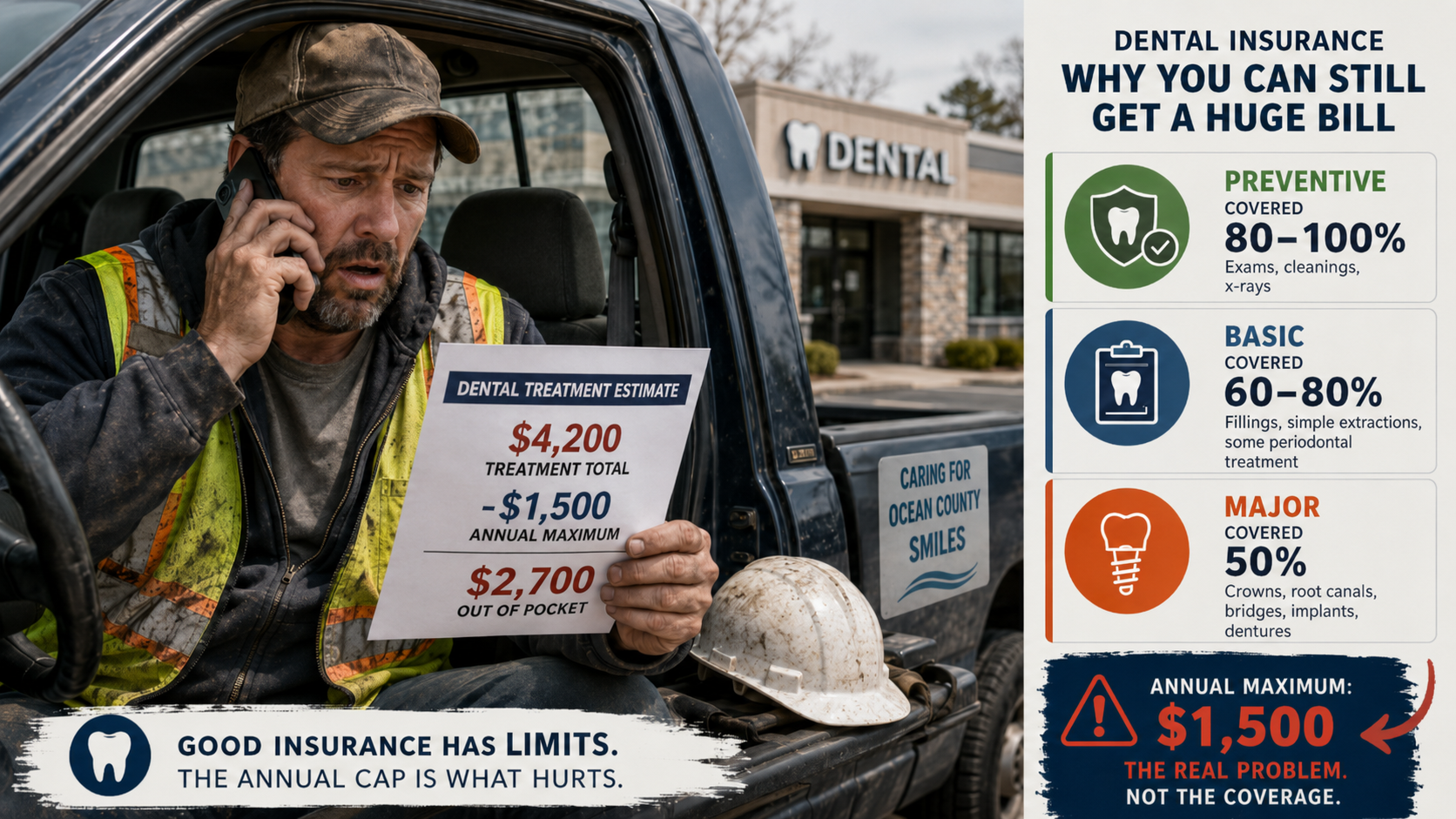
You Have Dental Insurance. Here Is Why It Does Not Work Like You Think.
A construction supervisor in Ocean County went to his dentist [...]

The Number That Controls Your Dental Care (And Has Not Changed Since Your Parents Were Kids
A teacher in Passaic County needed a crown [...]
How Dental Insurance Actually Works
It doesn’t work the way you think it does. And it isn’t your fault.
The $1500 Ceiling
 Imagine if your car insurance stopped paying after $1,500 a year. You would pay your premium every month, file a claim after an accident, and hear: “Sorry, you’ve used up your annual benefit. The rest is on you.”
Imagine if your car insurance stopped paying after $1,500 a year. You would pay your premium every month, file a claim after an accident, and hear: “Sorry, you’ve used up your annual benefit. The rest is on you.”
You would call that absurd. But that is exactly how most dental plans work.
The majority of dental plans cap what they will pay each year somewhere between $1,000 and $1,500. That ceiling has barely changed since the 1970s. Your premiums have gone up. The cost of dental care has gone up. The cap has not.
This means a single crown, a root canal, or an unexpected extraction can use up most of your annual benefit in one visit. Everything after that comes out of your pocket.
Dental Insurance Is Not Health Insurance
When you break your arm, your health insurance covers most of the bill. There might be a copay or a deductible, but the insurance is designed to protect you from catastrophic cost. That is the whole point.
Dental insurance is designed differently. It is built around a yearly payment ceiling and a tiered system that shifts more cost to you as treatment gets more serious. Preventive care like cleanings and exams is usually covered at 80 to 100 percent. Basic work like fillings drops to 60 to 80 percent. Major work like crowns, root canals, and dentures often drops to 50 percent. And that 50 percent still counts against your annual maximum.
The result: your dental plan is really a capped benefit with built-in cost-sharing. It helps with routine care. It was never designed to fully protect you when something goes wrong.
This Affects More People Thank You Would Think
The dental insurance system does not have a single point of failure. It has dozens. And they affect everyone, from the family earning six figures to the parent working two jobs.
If you earn $90,000 and your employer offers dental:
You probably have a plan with a $1,500 annual maximum. Your family hits that ceiling by April, then pays full price for anything else the rest of the year. You are insured. You are still stretching to afford care.
If you work in a warehouse, a restaurant, or a retail store:
Your employer may offer dental, but the plan might cap at $750 or $1,000 with higher copays. A single filling and a crown could exhaust your benefit. You have “coverage.” It barely functions.
If you were offered dental at work and said no:
You probably did the math. The premium was $40 to $60 a month for a plan that tops out at $1,500. If you only go for cleanings, you are paying more in premiums than you would pay out of pocket. That is not irrational – the math genuinely does not work for many people. But now you have no safety net if something goes wrong.
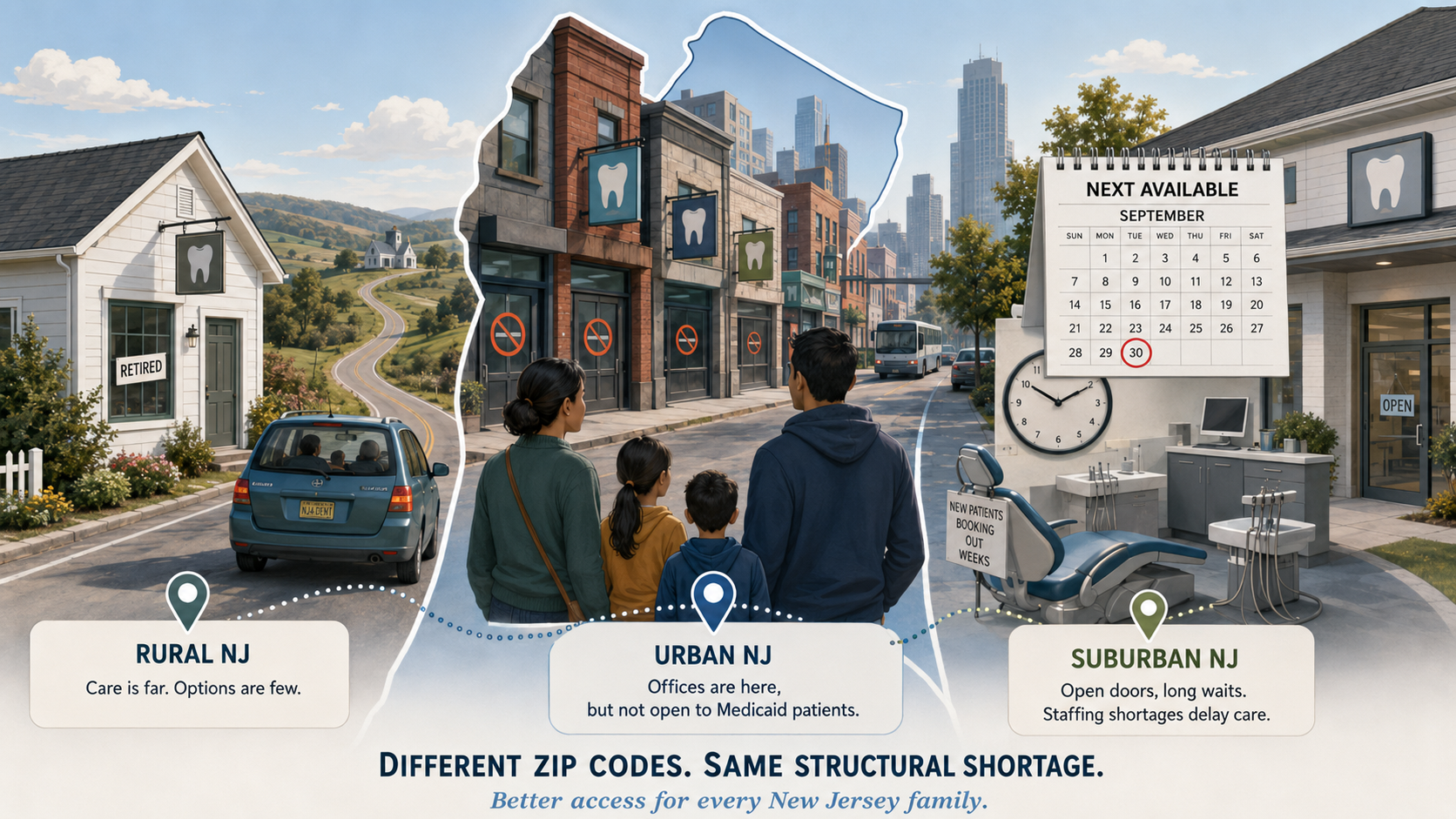
If you are on Medicaid:
You have a card that says you are covered. Finding a dentist who accepts it is a different story. In New Jersey, only about one in four dentists participate in Medicaid – not because they don’t want to help, but because the reimbursement often does not cover the cost of delivering care.
The system does not have a single point of failure. It has dozens. And they affect everyone.
The Paperwork No One Sees
Behind the scenes, your dentist’s office is doing something you never see: spending hours every week communicating with insurance companies. Filing claims. Waiting for approvals. Resubmitting denials. Navigating coding changes.
In New Jersey, more than half of dentists spend 40 or more hours a year – a full work week – just on insurance communications. That is time that is not going to patients.
The paperwork has become its own waiting room. And when administrative burden piles up, some dental offices make a rational decision: they stop accepting certain plans. Which means fewer in-network options for you.
What Can You Do About It?
The system is rigged in ways you didn’t create and can’t fix alone. But there are things you can do this week:
1. Before any procedure beyond a cleaning, ask: “How much of my annual maximum is left?” and “What will my estimated out-of-pocket cost be?”
2. If you’ve already hit your annual maximum, ask about phasing treatment across two benefit years.
3. If you’re on Medicaid and can’t find a dentist, start with community health centers (FQHCs). They accept Medicaid and use sliding-fee scales.
4. Learn what the words on your plan actually mean. (Link to the Glossary post in the feed below.)
5. Share what you’ve learned. Most people find out how dental coverage actually works only after something goes wrong. Help someone before they need to.
The Empty Chair

Walk into a dental office in New Jersey today and you might notice something the front desk doesn’t always mention. There is a hygiene room sitting empty. Maybe two of them. Not because no one needs a cleaning – the appointment book is full – but because there is no hygienist available to use those chairs.
The empty chair is the operational reality of NJ’s dental access problem. When you call your dentist’s office and hear that the next available appointment is three months out, this is usually why. The dentist is there. The space is there. The team needed to deliver care is not.
This is the second system that fails dental access in New Jersey. The first system is dental insurance, which traps coverage in caps and confusion. The second is the dentist-led care team itself – and right now, that team is stretched thinner than most patients realize.
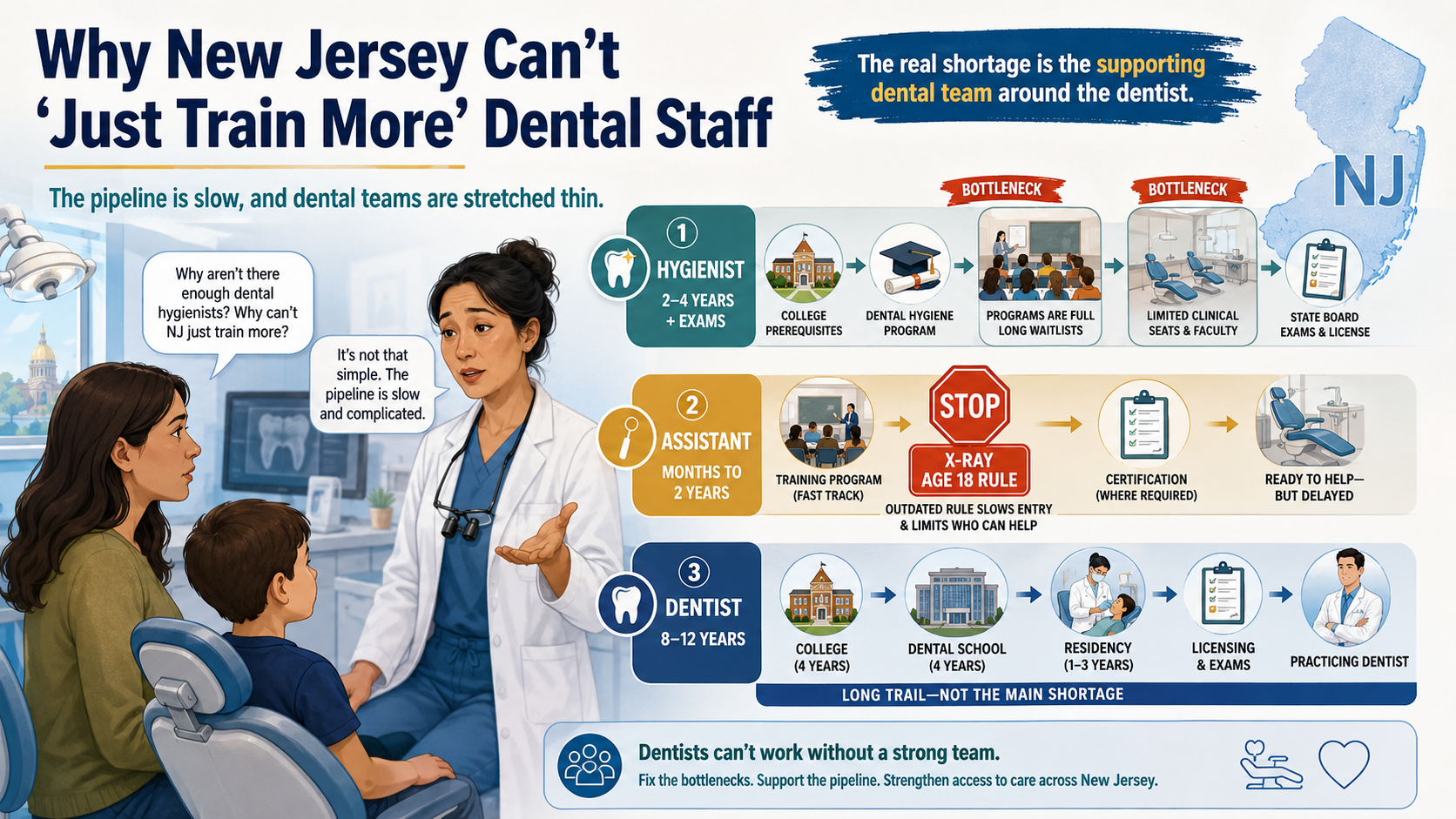
It Is Not A Dentist Shortage. It Is A Team Shortage
 Most patients say ‘there is a dentist shortage’ because that is the language they have absorbed from headlines. The actual operational reality in New Jersey is different. Dentists are graduating. NJ has dental schools producing new dentists every year. The dentist supply is roughly stable.
Most patients say ‘there is a dentist shortage’ because that is the language they have absorbed from headlines. The actual operational reality in New Jersey is different. Dentists are graduating. NJ has dental schools producing new dentists every year. The dentist supply is roughly stable.
What is not stable is the supply of dental hygienists and dental assistants – the members of the dentist-led care team who do the work that lets a dentist see more patients. Hygiene programs are at capacity. Dental assistant pipelines are blocked by an outdated state regulation that prevents 16- and 17-year-olds from training in supervised radiologic settings. Existing hygienists and assistants are leaving the field faster than new ones enter, often because rising wages are not keeping pace with the cost of living and the burden of administrative work.
The fix is not ‘train more dentists.’ The fix is expanding capacity within dentist-led practices by growing the team around the dentist – more hygienists, more assistants, more support staff working under dentist supervision so that more patients can be seen safely.
Until that team is whole, the chair stays empty.
What This Looks Like In Real Life
The team shortage does not show up as a single dramatic failure. It shows up as a hundred small ones, in dental offices across New Jersey, every day.
The Office That Stopped Offering Saturday Hours
A suburban dental practice in central Jersey used to see patients on Saturdays. Their hygienist who worked weekends took a job closer to home. They could not find a replacement willing to work Saturdays at the wage they could afford to pay. Saturday hours quietly disappeared. Patients who work weekdays now have nowhere local to go on the weekend.
The Cleaning That Is Now 2 Months Out
A family practice in northern Jersey has two hygienists on staff and needs three. The third position has been open for eight months. Every cleaning the practice books is now scheduled two months further out than it would have been three years ago. Patients with painful problems are waiting longer than the patients who scheduled ahead.
The Medicaid Contract That Had To End
A practice in a high-need community south of Trenton used to accept Medicaid patients. They had a dental assistant trained specifically for higher-volume patient flow that Medicaid required. When that assistant left, the practice could not replace her. They had to stop accepting new Medicaid patients. The dentist still wanted to help. The team to support was not there.
The rural community with one position open for a year.
A solo dentist in the northwest part of the state has had a hygienist position open for over a year. Three towns away, another solo dentist has the same problem. The hygiene program at the nearest college has a waiting list. Even if a graduate were available tomorrow, the rural commute and lower wage scale make it hard to fill these positions.
Every empty chair is a patient not getting seen.
Every patient not getting seen is a small piece of dental access disappearing.
Why The Pipeline Is Slow
When people hear there is a workforce shortage, they often ask: why not just train more? Here is why it is not that simple.
Dental hygienist programs in NJ are 2 to 4 years long. Existing programs are at capacity for faculty and clinical placement spots – they cannot just add more students next semester.
Dental assistant pipelines through career and technical education are blocked by an outdated NJ regulation requiring trainees to be 18 to operate dental X-ray equipment, even under direct dentist supervision. This shuts out high school CTE programs that could be feeding the dentist-led care team for years.
Even when programs grow, training takes time. The team shortage is real today. The solutions take years. This is why expanding capacity within dentist-led practices is the immediate answer, not pipeline growth alone.
How To Help Your Dental Care Team
The team shortage is bigger than any one patient can fix. But there are things you can do this week that make life easier for your dentist’s office and protect your own access to care.
1. Book preventive visits as far in advance as possible. The earlier you reserve a slot, the more likely you get the time you want.
2. Ask about cancellation lists. Many offices keep one. If you can come in on short notice, you can fill an opening someone else dropped.
3. Show up on time and ready. Late arrivals and last-minute cancellations stress already-thin schedules. Your reliability helps the whole team.
4. If you cannot find an in-network appointment in your area, consider community health centers or dental school clinics, where the staffing situation is sometimes different. (See Find Care for options.)
5. Be patient with the front desk. They are working with the resources they have and they are doing their best.
What Is Being Done About It
These problems did not happen overnight and they will not be fixed overnight. But they are not being ignored.
Right now, there are proposals being considered in New Jersey that would address both systems – from raising reimbursement so more dentists can afford to say yes to patients on public coverage, to removing outdated barriers that prevent young people from entering the dentist-led care team through career training programs.
When those proposals are ready for your voice, you will find them on our [Take Action] page (Coming Soon).
In the meantime, the stories and explanations below are here to help you understand what is happening – and what you can do to protect yourself and your family while the system catches up.