Here are four people in New Jersey. All of them are dealing with the same dental insurance system. None of them are doing fine.
The project manager in Monmouth County
She earns $95,000 a year. Her employer offers what she always assumed was good dental coverage. Her plan has a $1,500 annual maximum per person – the most the plan will pay for each covered family member in a year.
Her husband and two kids each have their own separate $1,500 limit. On paper, that sounds like $6,000 in family dental benefits. But that is not how it works.
Each person’s maximum is separate. Her husband cannot use hers. She cannot use her kids’. If one person has a bad dental year, that person hits the wall alone.
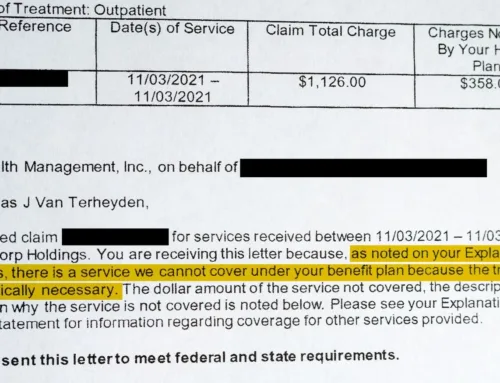
In March, she needs a crown. The crown costs $1,400. Her plan covers major services at 50 percent, so the plan pays $700 and she pays the other $700 out of pocket. That $700 the plan paid also counts against her own $1,500 annual maximum.
In September, she needs a root canal and buildup on another tooth. The total cost is about $1,700. Her plan would normally cover 50 percent, but by then she only has about $800 left under her annual maximum. The plan pays what is left. She owes the rest.
Her husband’s maximum is untouched. Her kids’ maximums are untouched. But she cannot borrow from theirs. Their unused benefits sit there while her own limit runs out.
She has insurance. She is insured. But one difficult year with her teeth means she is paying hundreds, and possibly thousands, out of pocket – even while her family has thousands of dollars in unused benefits sitting right there, unusable.
The warehouse worker in Middlesex County
He works full time at a distribution center. His employer offers dental coverage, but the plan caps at $750 per person per year with higher copays than the project manager’s plan. His maximum is half of hers before anything even happens.
One filling and one crown in the same year could exhaust most or all of his benefit. He has had a toothache for three weeks and has been putting off the call because he already knows the answer: whatever is wrong is probably going to cost more than his plan will cover. If he needs a crown, his $750 maximum will barely make a dent in the bill. The rest comes from a paycheck that is already stretched.
He has “coverage.” But it barely functions as protection. And unlike the project manager, whose plan at least covers routine care comfortably, his copays are high enough that even a cleaning costs him real money.
The home health aide in Camden County
She was offered dental insurance at open enrollment last fall. She sat down with the paperwork and did the math.
The premium was $55 a month – $660 a year out of her paycheck. The annual maximum was $1,500. The deductible was $100.
For the past five years, she had only gone to the dentist for cleanings. If she did the same thing this year, she would pay $660 in premiums for roughly a few hundred dollars’ worth of routine care. The plan might cost her more than it paid.
She declined the coverage. It was not a careless decision. It was a rational choice inside a system that gave her bad options. The product was designed for someone who expects to need major work and can afford the premium in the meantime. For someone who only needs routine care, the premium can feel impossible to justify – until something goes wrong.
But now she has no safety net. If a tooth cracks next Tuesday, she is paying for everything herself. And she does not have $1,400 for a crown sitting in a savings account.
She is not irresponsible. She made the only decision the math supported. The system just does not offer her a good one.
The factory worker in Hudson County
She works at a packaging plant and has NJ FamilyCare – Medicaid coverage for herself and her two children. The card in her wallet says she is covered. Finding a dentist who accepts it has been a different experience entirely.
She has called six offices in her neighborhood. Two said they do not take Medicaid. One had a number that was disconnected. Two could not see new Medicaid patients for several months. The sixth said they could see the kids but not her – they only accept Medicaid for pediatric patients.
She has coverage. She has proximity. She does not have access.
And the reason is not as simple as dentists wanting or not wanting to help. In New Jersey, Medicaid dental reimbursement often falls far below the actual cost of delivering care. For many private dental offices, participation becomes financially unsustainable. The decision is not between helping and not helping. It is between absorbing losses on every visit or keeping the practice open for the patients they can still serve.
Her Medicaid card says she has dental coverage. But a benefit that exists on paper does not always translate into an appointment.
The common thread
Four people. Four income levels. Four different relationships with dental coverage.
The project manager’s ceiling has not moved since the 1970s. The warehouse worker’s ceiling is even lower. The home health aide’s premiums have risen while the benefit has not. And the factory worker’s Medicaid card opens a door that most dental offices in her neighborhood have had to close.
All of them are caught in the same system: one built around annual maximums, coverage tiers, deductibles, copays, and reimbursement rates that often do not reflect the real cost of dental care today. A $1,500 maximum may sound meaningful until one crown, one root canal, or one emergency uses most of it up. And that number has barely changed in over fifty years.
This is not a story about people who cannot afford insurance. It is a story about a system where having insurance – or having coverage – does not always mean having enough.
What you can do no matter which of these sounds like you
If you have employer coverage, check your annual maximum now – not after something goes wrong. Each person on your plan has their own separate limit. One family member usually cannot use another’s unused benefits. Call your benefits office or look at your plan summary. Know the number for yourself and for every person covered.
Before any major procedure, ask two questions: “How much of my individual annual maximum is left?” and “What will this cost me out of pocket?” You deserve to know those answers before treatment begins, not after the bill arrives.
If you need multiple procedures and your annual maximum is running low, ask your dentist whether the treatment plan can be scheduled across two benefit years in a clinically appropriate way. Do not assume that starting a crown in one year and finishing it in another will automatically split the benefit. Many plans count a crown based on the completion or cementation date. But when several procedures are needed, timing may matter – and your dentist’s office can help you think through the options.
If you were offered dental coverage and declined it, revisit the math at your next open enrollment. Some employers offer more than one plan tier, and the calculation changes if you expect to need anything beyond routine cleanings. If the math still does not work, you are not wrong – but know that community health centers and dental school clinics may offer care for uninsured patients, often on sliding-fee scales. You have options even without a plan.
If you are on Medicaid and cannot find a dentist, start with community health centers. They accept Medicaid by design and often serve patients regardless of income. Our Find Care page can help you locate one near you. Do not give up after three calls. Directories can be outdated, phone numbers can be wrong, and not every listed office is actually taking new patients. The care may still be out there – but too often, patients have to fight through a broken system just to find it.